For a printable version please see: URINARY TRACT ANOMALIES
URINARY TRACT ANOMALIES IN CHARGE: FOR THE UROLOGIST
Marc S. Williams, M.D., Department of Pediatrics, Gundersen Lutheran Medical Center 1836 South Ave., LaCrosse, WI 54601 [email protected]
(608)782-7300 X2363
TYPE AND FREQUENCY OF URINARY TRACT ANOMALIES IN CHARGE SYNDROME
◆ 20-40% have a urinary tract anomaly (1,4).
◆ All types of structural problems (solitary kidney, hydronephrosis, renal hypoplasia, duplex kidney, posterior urethral valves, etc.) have been reported, as well as vesico-ureteral reflux.
◆ Facial palsy is significantly associated with renal anomalies, which are usually ipsilateral to the palsy (2)
◆ Children with CHARGE are at increased risk for urinary tract infection. Evaluation of a patient who has fever without a source should include a urinalysis and urine culture.
Diagnostic tests
1. Baseline renal and bladder ultrasound to evaluate anatomy are warranted, as early identification and treatment may reduce long-term morbidity (3,4).
2. Functional studies (such as voiding cystourethrogram) may be indicated as follow-up to anatomic study, or if the patient develops urinary tract infection.
Medical management and caveats
1. Standard medical therapy is acceptable for treatment of UTIs. Suppressive therapy may be necessary if infections are recurrent.
2. Surgical intervention is indicated for certain abnormalities. Indications for surgery are the same as for children who don’t have CHARGE. Caveats for surgery include:
a. Anesthetic risk is increased in children with airway involvement such as choanal atresia or laryngotracheomalacia (both common in CHARGE). Children with choanal atresia and complex heart defects have the highest rate of serious complications and/or poor outcome.
b. Swallowing problems with increased secretions (presumably due to involvement of cranial nerves IX and X) may present an additional risk of aspiration.
D. References
1. Tellier AL, Cormier-Daire V, Abadie V, et al. CHARGE Syndrome: Report of 47 cases and review. Am J Med Genet 1998;76:402-409.
2. Blake KD, Russell-Eggitt IM, Morgan DW, et al. Who’s in CHARGE? Multidisciplinary management of patients with CHARGE association. Arch Dis Child
1990;65:217-233.
3. Blake KD, Davenport SLH, Hall BD, et al. CHARGE Association: An update and review for the primary pediatrician. Clin Pediatr 1998;37:159-174.
4. Ragan DC, Casale AJ, Rink RC, Cain MP, Weaver DD. Genitourinary anomalies in the CHARGE association. J Urology 1999;161:622-625.
THE URINARY TRACT IN CHARGE SYNDROME: PARENT INFORMATION
Marc S. Williams, M.D., Department of Pediatrics, Gundersen Lutheran Medical Center 1836 South Ave., LaCrosse, W1 54601 [email protected] (608)782-7300 X2363
STRUCTURE AND FUNCTION OF THE URINARY TRACT
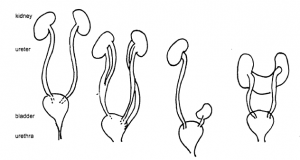
| Normal |
duplicated |
pelvic (ectopic) |
horseshoe |
| urinary |
ureters |
kidney |
kidney |
| system |
The normal urinary tract consists of two kidneys. Urine is produced in the kidney and is drained by the renal pelvis. Urine then flows into the ureters. These tubes drain into the urinary bladder. When we urinate, the urine travels through another tube called the urethra. This tube is very short in females and longer in males (as it has to travel through the length of the penis). Urine normally only flows in one direction.
URINARY TRACT ABNORMALITIES IN CHARGE
Abnormalities of the urinary tract are seen in 20-40% of children with CHARGE syndrome. They can be of two types, structural or functional.
Structural abnormalities (urinary tract isn’t formed properly).
1. Absent or hypoplastic kidney – one kidney is not present or small. 1f a child is missing both kidneys they cannot survive.
2. Ectopic, or pelvic kidney – kidney is in an abnormal location, much lower than it should be.
3. Horseshoe kidney – the two kidneys are joined together to make one kidney shaped like a horseshoe.
4. Duplications (kidney, renal pelvis and/or urethra can be partially or completely duplicated). Obstruction to urinary flow is frequently seen.
5. Hydronephrosis or enlargement of the renal pelvis – excess fluid into the kidneys. This can be caused by a blockage between the renal pelvis (kidney) and the urethra (which is called a ureteropelvic junction, or UPJ obstruction), or by severe vesicoureteral reflux (see below).
Functional abnormalities (urine doesn’t flow properly)
1. Vesicoureteral reflux (hereafter referred to as reflux). When the bladder contracts to assist urination, urine normally flows out the urethra. The bladder wall pinches off the ureters to prevent urine flowing backwards towards the kidneys. 1f the ureters remain open during bladder contraction, urine can flow back towards the kidney. This is reflux. 1t can be mild to severe. Reflux can predispose to urinary tract infection (UT1). 1f severe, it can result in hydronephrosis and direct damage to the kidneys, which can ultimately lead to kidney failure.
2. Bladder residual. Bladder does not empty completely. This can predispose to urinary tract infections.
DIAGNOSTIC TESTS
1. Renal Ultrasound identifies structural abnormalities.
2. Voiding Cystourethrogram (VCUG) This test is indicated if reflux is suspected. 1t involves placing a small tube (catheter) through the urethra into the bladder. The bladder is filled with a liquid that can be seen on X-ray (contrast). X-rays are taken while the child urinates. This test is necessary to diagnose reflux or bladder residual.
3. 1ntravenous Pyelogram (1VP) This is another test primarily used to examine kidney structure. Because it involves the injection of contrast into a vein as well as X-ray exposure, this test has for the most part been replaced by the renal ultrasound. 1t does have the advantage of requiring intact blood supply to the kidneys and provides information regarding the kidney’s ability to make urine (which neither #1 or #2 do). 1VP can be used to determine if duplicated kidneys are functioning.
4. Radionucleotide renal scan. This test involves the injection of a radioactive material into a vein that concentrates in the kidney. 1ndications for the test are similar to #3, but this test gives more information about function and less information about structure than the 1VP. The amount of radioactive is small and it is rapidly eliminated in the urine so radioactivity dose is small.
5. Computerized tomography (CT) and Magnetic Resonance 1maging (MR1). Both of these tests provide high-resolution images that allow much better definition of structure than the renal ultrasound. One of these would be indicated if the renal ultrasound was unable to resolve a complex structural abnormality of the urinary tract. The CT scan uses X-rays, but usually does not require sedation as it scans very rapidly. The MR1 uses magnetic fields (which do not have harmful effects on body tissues) and has better resolution than CT scan. 1t can also be used to evaluate blood vessel anatomy (Magnetic Resonance Angiography or MRA). The scan time is longer, so young child frequently requires sedation. This is an important issue in CHARGE children due to the increased risk of airway compromise (see section 5f). We recommend full airway precautions, as discussed elsewhere, if sedation is to be used.
MANAGEMENT OF URINARY TRACT ABNORMALITIES
1. All CHARGE children should have a baseline renal ultrasound done in infancy looking for structural abnormalities.
2. Any child who has fever without an identifiable source on physical examination should have a clean urine specimen obtained looking for UT1. This may involve placing a catheter through the urethra to obtain a specimen or sticking a needle through the abdomen into the bladder (suprapubic or bladder tap). Bagged specimens are inadequate for this purpose. Older children may be able to provide a clean voided specimen. Urine culture must be done to confirm UT1.
3. UT1s can be treated with standard antibiotics. A documented (urine culture positive) UT1 is an indication for VCUG.
4. Recurrent UT1s may require use of a daily antibiotic. This is called suppressive or prophylactic therapy. 1f a VCUG has not been done, it must be done at this point.
5. Surgery is indicated to correct some structural anomalies, and may be indicated in severe cases of reflux. An urologist with pediatric experience should assist with this decision. Follow all surgical and anesthetic precautions as discussed elsewhere.
OUTCOME
Aggressive medical and surgical intervention should be able to prevent or treat most complications of these abnormalities. Rarely, anomalies may be so severe as to inevitably progress to end stage renal disease (ESRD also known as kidney failure), which may necessitate consideration of dialysis or kidney transplant. There is only a single report in the medical literature of this occurring in CHARGE syndrome. (This was in an adult in whom CHARGE syndrome was not recognized until he presented in renal failure. The authors felt that if the syndrome had been recognized early on, diagnostic test could have been done that may have prevented the renal failure).